
Corneal Disorders
26 January 2026 2026-02-16 11:30Corneal Disorders


CXL: Corneal Collagen Cross Linking
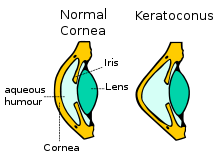
A new therapeutic approach for the treatment of keratoconus is the interconnection of the corneal collagen (Corneal Cross Linking, CXL) with the use of riboflavin (vitamin B2) and Ultraviolet irradiation A. The aim is the improvement of the resistance and rigidity of the cornea -stiffening effect- that ceases the development of keratoconus. IVO in this moment is concerned as the world’s avant-garde in the application of this treatment and constitutes a point of reference in CXL treatment.
A one-time application of riboflavin solution is administered to the eye and is activated by illumination with UV-A light for approximately 30 minutes. The riboflavin causes new bonds to form across adjacent collagen strands in the stromal layer of the cornea, which recovers and preserves some of the cornea’s mechanical strength. The corneal epithelial layer is generally removed in order to increase penetration of the riboflavin into the stroma.The duration of the treatment is one hour and it is painless due to the use of local anesthaetic drops. In the end of the treatment, a bandage contact lens is placed in the eye which remains from 4 to 6 days.

INTACS
The INTACS (Intrastromal Corneal Ring Segments or Intracorneal rings) are small rings of biocompatible material, which are placed in the cornea of the patients with keratoconus in order to improve the topographic images and the visual acuity of the patients.
The placement of the rings demands the creation of a tunnel in the cornea with the use of a 5th generation Laser the iFS Advanced Femtosecond Laser and the patient does not feel them in his eye at all. The placement of Intacs is decided by the surgeon depending on the particular characteristics of each patient. The intervention is conducted under anesthaetic drops and is painless.

Lamellar and Penetrating Keratoplasty
Lamellar and Penetrating keratoplasties are interventions in which total or partial transplantation of the corneal tissue is effectuated for the treatment of various diseases of the cornea that considerably decrease visual acuity.
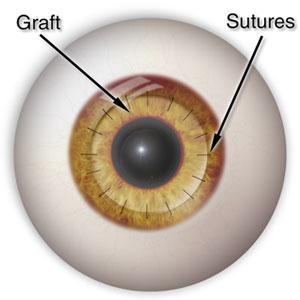
Keratoplasty can be penetrating (full corneal transplantation) or partial, such as lamellar keratoplasty or endothelium transplantation (DSAEK). Until recently, incisions were made by the use of specially designed surgical instruments which resulted in the need of stitches and high postoperative astigmatism. At LVO those incisions can be performed with the use of the Femtosecond Laser offering numerous advantages. Firstly, we can precisely create the same dimension implant in both donor and recipient corneas and moreover we can give various different shapes. The result is fewer stitches, less post operative astigmatism and graft form depending on our patients needs.
![]()
At IVO as well as at the University Hospital Ophthalmology department, apart from the common keratoplasty methods, partial anterior and posterior keratoplasty are performed. These modern applications have good results in respect to the conventional keratoplasty because keratoconus, trauma, corneal scars and enthodethium pathology can be confronted successfully with the use of the Femtosecond Laser.
